News Don’t drink
Nipah Virus: Don’t drink raw date juice
Warns IEDCR as country reports this year’s first death
Health experts yesterday advised people to not drink raw date juice, the main source of the Nipah virus in the country, following the recent death of a woman.
At an event yesterday, the Institute of Epidemiology, Disease Control and Research (IEDCR) told reporters that the 35-year-old woman died from Nipah-induced encephalitis in Rajshahi last week.
Last year, the IEDCR recorded three Nipah virus cases, two of which led to death – one in Naogaon and the other in Faridpur.
"We don't know much about this deadly virus yet. So far, we know that it has around 71 percent fatality rate and raw date juice is the main source of contracting it. So, we must refrain from consuming it," said Prof Tahmina Shirin, director of the IEDCR, while sharing data on the viral infection.
She, however, said consuming the juice of dates or molasses is safe when and if it is boiled [as high temperatures may kill the virus].
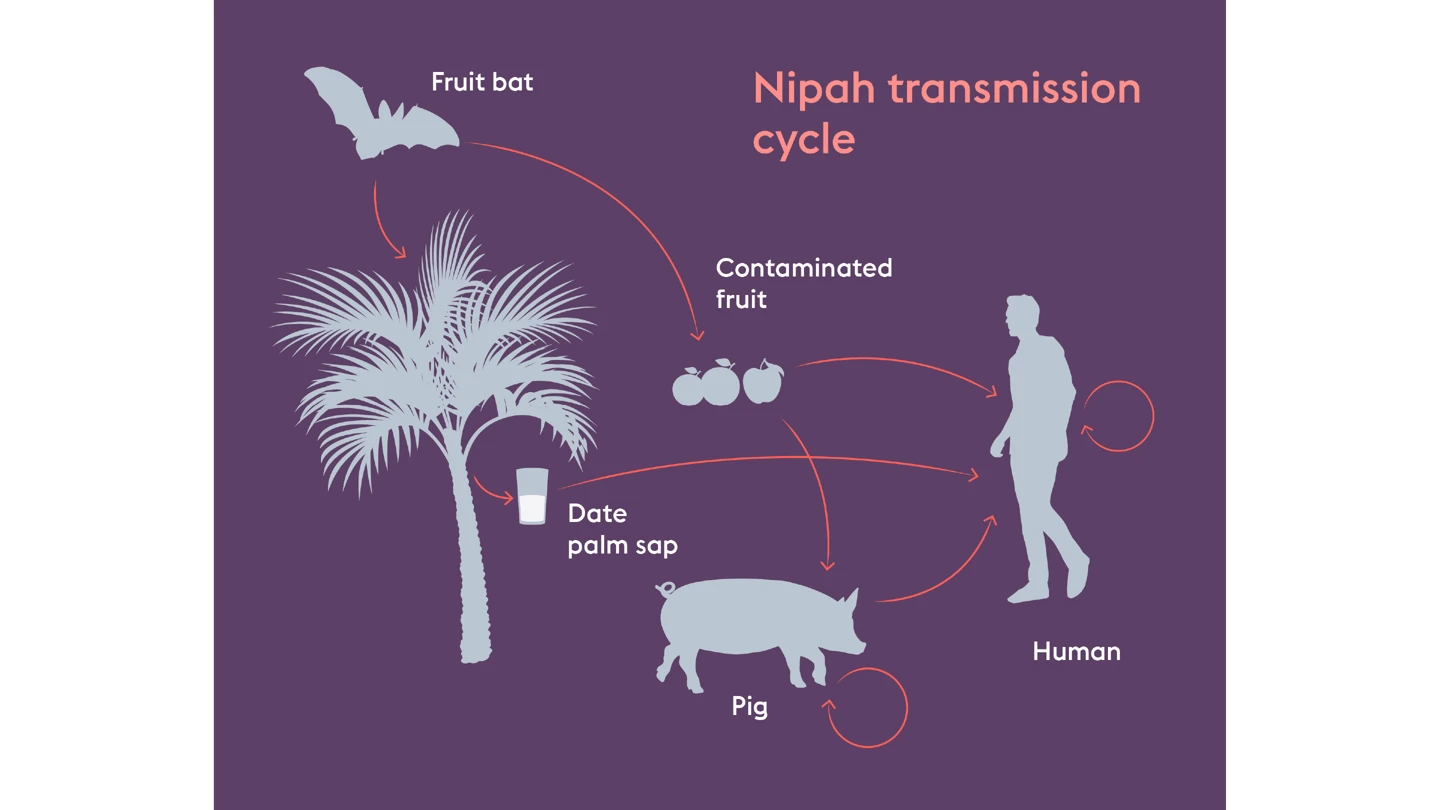
According to the World Health Organization, the Nipah virus infection is a zoonotic illness that is transmitted to people from animals and can also be transmitted through contaminated food or directly from person to person.
It causes a range of illnesses from asymptomatic (subclinical) infection to acute respiratory illness and fatal encephalitis. The virus can also cause severe diseases in some animals.
In Bangladesh and India, the consumption of fruits or fruit products (such as raw date palm juice) contaminated with the urine or saliva from infected fruit bats were the likeliest sources of the virus.
According to the IEDCR, infected people initially develop symptoms such as fever, headaches, myalgia (muscle pain), vomiting and sore throat. An undetected patient can even fall into a coma within 24 to 48 hours of contracting the virus.
There are currently no drugs or vaccines that specifically target Nipah virus infection. The primary treatment for humans is supportive care.
Dr Sharmin Sultana, senior scientific officer at the IEDCR, presented the highlights on Nipah surveillance in Bangladesh.
The virus was first identified as the cause of an encephalitis outbreak in 2001 in Meherpur.
In 2006, the Nipah Surveillance and Laboratory was established at the IEDCR.
Since then, 330 cases of the infection were documented. Of those infected, 231 died, indicating a very high mortality rate – 71 percent.
At least 139 of those infected contracted it from bats through date juice, while 46 others from another human carrier.
Closing in on protection against deadly Nipah virus
Nipah virus is among the world’s deadliest pathogens, yet no approved countermeasures currently exist. CEPI is working to change that through its $150 million Nipah virus R&D portfolio spanning the full preparedness chain—from countermeasure development and manufacturing to anticipating a Nipah-like Disease X from the same paramyxovirus family—including funding the world’s most advanced Nipah vaccine candidate, now in Phase II trials in Bangladesh.
For this Innovations for Impact story, we spoke with icddr,b’s Dr K Zaman, who is leading the first-ever Phase II Nipah vaccine trials, and CEPI’s Nipah programme lead, Rick Jarman, to explore how CEPI is helping the world prepare to confront one of the most lethal viral threats.
___________
Fruit juice—seemingly harmless and enjoyed the world over. But for some people in Bangladesh, drinking a popular local juice can come with deadly consequences.
“Raw date juice is a well-enjoyed drink among rural communities in Bangladesh. But many don’t realise it can be contaminated by bats who carry the Nipah virus,” said Dr K Zaman, Principal Investigator of the first-ever Phase II CEPI-funded Nipah vaccine trial at Bangladesh’s icddr,b, a health research institution. “People drink the juice and become infected.”
This simple thirst-quenching accident can prove fatal. Nipah virus kills up to 75 percent of the people it infects. It is one of the world’s most lethal viral pathogens.
It’s this extremely high death rate, and the fact that Nipah has the potential to mutate and spread to many more parts of the world, that is driving scientists to develop a protective vaccine.
One potential vaccine, developed in a CEPI-funded partnership with the University of Oxford and its ChAdOx vaccine platform, was the first in the world to begin mid-stage clinical trials in Bangladesh in late 2025.
Dr Zaman, who has overseen 78 clinical trials at icddr,b, said he hopes this trial will generate new knowledge on how a future Nipah vaccine could save lives in Bangladesh.
And it’s not just Bangladesh that could one day benefit from this vaccine. Since its discovery in 1998, Nipah outbreaks have been confined to South and Southeast Asia. But the virus’s natural hosts—fruit bats—range across regions that are home to more than two billion people. As human activity pushes deeper into bat habitats, the risk of spillover is only growing.
Rick Jarman, Nipah programme lead at CEPI, said the fact that such a large range of domestic and farm animals are susceptible to Nipah virus from bats is a major concern, as Nipah can infect humans both through contaminated food and direct contact with infected animals. Each time it spills over, the risk of mutation and potentially increased transmissibility grows, he said.
CEPI is the world’s largest funder of Nipah research and development. Its $150 million portfolio—including two Nipah vaccine candidates and a monoclonal antibody—spans the whole preparedness chain, from countermeasure development and manufacture, to preparing for a novel Nipah-like Disease X—an as-yet unknown pathogen with outbreak potential—that could emerge from the same paramyxovirus viral family.
A big part of this preparedness comes from CEPI’s partnership with the University of Oxford and Serum Institute of India—the world’s largest vaccine manufacturer and part of CEPI’s Vaccine Manufacturing Network. This collaboration not only enabled Serum to manufacture Oxford’s ChAdOx1 NipahB vaccine candidate for the Phase II Bangladesh trials, but it also aims to create an investigational-ready reserve of up to 100,000 doses of the vaccine. These doses could then be deployed under a research protocol in an outbreak.
Jarman described this investigational reserve as CEPI’s “number one priority” for Nipah virus over the next year or two. With the potential for experimental vaccine doses at the ready in a region where the virus persistently pops up, it becomes possible to launch an emergency trial that can advance the candidate toward licensure and potentially – if the vaccine is indeed effective – provide protection to high-risk individuals.
The collaboration with Serum goes “way beyond being a manufacturing partner”, Jarman said and includes working with a world-class vaccine developer with deep regulatory experience and a strong relationship with the Indian government, alongside the regional experience required to make a Nipah vaccine a reality.
That’s important because large-scale efficacy trials, typically needed before a vaccine can be approved, are unlikely to be feasible given that outbreaks of Nipah are small and sporadic. But the potential data generated if the vaccine is used in emergency settings can help provide an alternative path to approval.
Jarman estimates that a Nipah vaccine could be ready for licensure within the next five years, so building these pathways with regulators now is crucial.
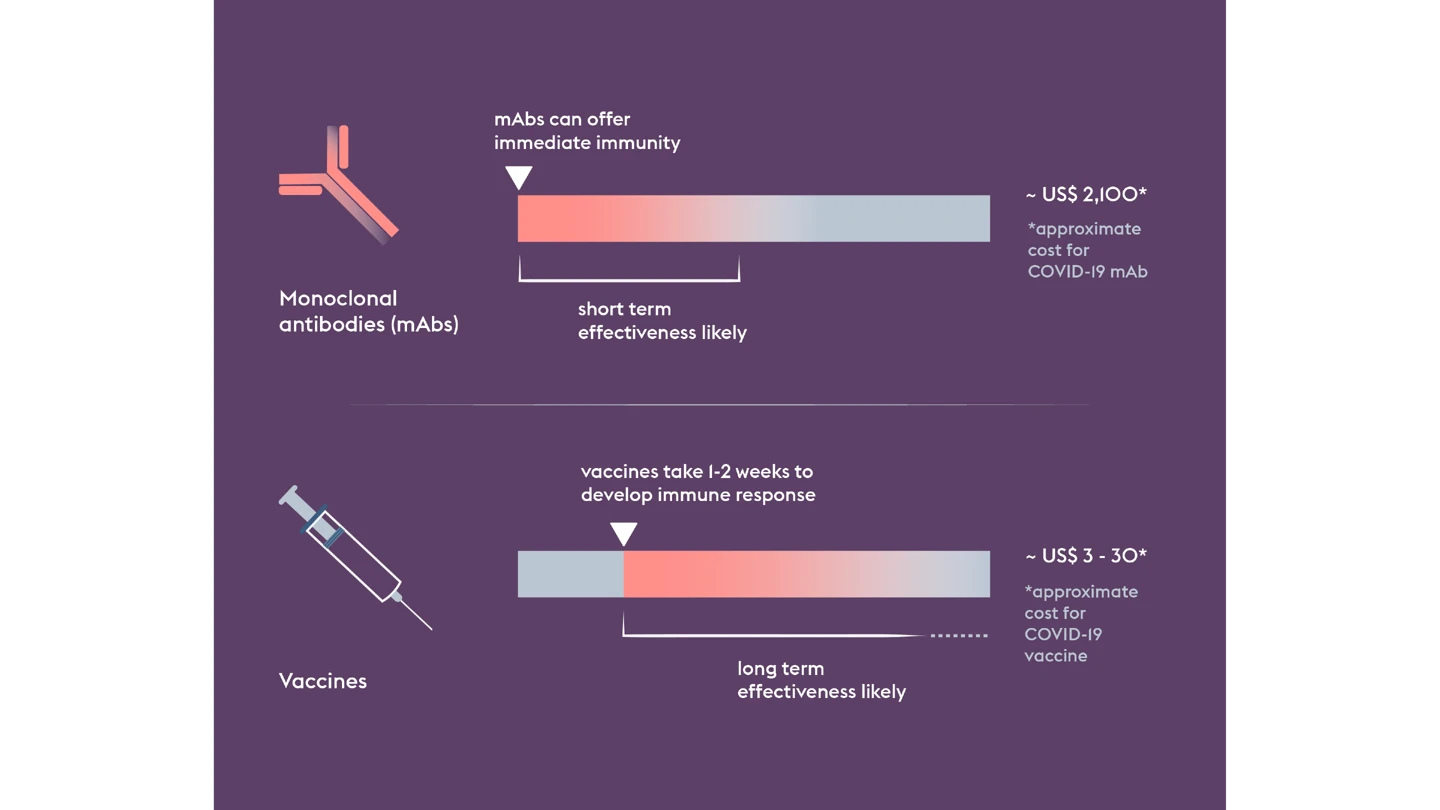
But when it comes to one of the world’s deadliest viruses, vaccines are only part of the story. Even if a vaccine proves successful, it could take weeks before someone vaccinated develops enough protective immunity.
That’s why CEPI is also funding the development of a Nipah monoclonal antibody, or mAb, which could provide immediate protection, acting as a bridge before the onset of longer-lasting vaccine-induced immunity. Such a tool would be particularly useful for protecting high-risk people like healthcare workers.
In what will be another world first, the Nipah mAb, MBP1F5, led by non-profit biotechnology company ServareGMP, is due to begin early to mid-stage trials in a Nipah-affected country in 2026.
Used together—vaccines and mAbs—they could provide a potent protective shield and constrain an outbreak’s potential.
Investing in a range of novel technologies and modalities like this increases the likelihood of successful countermeasure development and helps validate the technology for a future Disease X.
And it helps strengthen global preparedness against not only Nipah virus, but the entire paramyxovirus viral family. If a future paramyxovirus Disease X were to emerge, rapid response platforms like ChAdOx could be quickly adapted to create new vaccines, building on the scientific knowledge and data generated from Nipah R&D. Combined with regional manufacturing capability and expertise, this could accelerate the development of life-saving vaccines against an emerging paramyxovirus with epidemic or pandemic potential. This supports CEPI's 100 Days Mission, which aims to accelerate vaccine timelines to 100 days in response to a pandemic pathogen being identified.
Together, these strands of preparedness—countermeasure development, manufacturing and preparing for a Disease X—form a chain that could one day stop a future Nipah outbreak in its tracks and, at the same time, reduce the threat of other viruses lurking within the pernicious paramyxovirus family.
A 13-year-old girl was brought to the emergency room pregnant and revealed the truth to the doctor: “It’s my stepfather’s… He told me not to tell anyone…psss
A 13-year-old girl was brought to the emergency room pregnant and revealed the truth to the doctor: “It’s my stepfather’s… He told me not to tell anyone…
The moment Dr. Eleanor Hayes entered the emergency room, she immediately sensed something was wrong. The nurses looked shaken, whispering urgently as a pale, trembling 13-year-old girl sat on the exam bed, clutching the sleeves of her oversized sweatshirt. But nothing could have prepared Dr. Hayes for what would happen when she gently asked the girl her name.
“My name is Lily Carter,” the girl whispered, her voice barely audible. “And… I think I’m pregnant.”
Those words alone would have been heartbreaking. But it was what came next—her voice cracking, tears spilling down her cheeks—that froze the entire room.
“It’s… my stepfather’s,” Lily said. “He told me not to tell anyone… He said no one would believe me.”

That sentence hit Dr. Hayes like ice water. The main truth—raw, horrifying, life-changing—was out in the open from the very first minutes. And Lily wasn’t lying. The fear in her eyes was too real, too old for someone her age. Her hands shook violently as she hugged herself, bracing for punishment rather than help.
Dr. Hayes pulled up a chair, meeting Lily’s terrified gaze. “You did the right thing by telling me. You are safe now,” she said gently, even as her own heart pounded with anger and grief.
Lily explained that her mother worked night shifts, rarely home before sunrise, and her stepfather, Daniel Whitmore, used that time to control and manipulate her. Lily had tried to tell her mother once, but Daniel twisted the story, convincing her mother that Lily “made things up for attention.” After that, Lily stopped trying. She swallowed the fear, the shame, the isolation—until the morning she woke up with sharp stomach pain and collapsed at school.
A teacher called 911, and Lily was brought straight to the emergency room.
As the truth unfolded, Dr. Hayes discreetly signaled the hospital social worker, already knowing this would trigger a mandatory report and a chain of events that could completely destroy—or finally save—the little girl sitting in front of her.
For the first time since entering the ER, Lily’s voice steadied slightly. “Am I in trouble?” she whispered.
“No,” Dr. Hayes said firmly. “But someone else is.”

Within minutes, the hospital’s social worker, Marissa Doyle, joined Dr. Hayes in the small consultation room. They both knew the protocol: treat Lily’s immediate medical needs, secure her safety, document everything, and contact Child Protective Services and law enforcement.
But the emotional reality was far more delicate.
Lily flinched at every sound in the hallway. When Marissa introduced herself, Lily asked the same question over and over: “Are you sure he can’t come in here? He always shows up. He always finds me.”
Marissa reassured her that the hospital had already placed a security alert on her file. No unauthorized visitor would get near her.
As they continued the interview, Lily revealed how long the abuse had been happening, always describing events in vague terms, too afraid and too ashamed to repeat anything explicitly. Even without details, the truth was unmistakable—and devastating.
Dr. Hayes ordered an ultrasound, and when the screen lit up, Lily turned her face toward the wall. She didn’t cry. She didn’t move. She simply went numb.
“Lily,” Dr. Hayes said softly. “You are not responsible for this. None of this is your fault.”
“I don’t want him to hurt Mom,” she whispered. “That’s why I stayed quiet.”
Those words cut deeper than anything else. This child had been carrying the weight of a secret that would destroy most adults.
Meanwhile, the police had already arrived. Officer Raymond Porter and Detective Hannah Miller stood outside the room, reviewing the initial report. When they stepped inside, they approached Lily with the same gentleness Dr. Hayes had shown.
“Lily,” Detective Miller said, kneeling beside her, “we’re here to protect you. And we’re going to make sure he never hurts you again.”
Lily hesitated—but then gave a tiny nod.
When her mother, Catherine Whitmore, finally arrived at the hospital, she rushed into the room—only to be stopped by police. At first, she was confused, then horrified, then shattered when she learned the truth. She collapsed, sobbing, apologizing over and over for not seeing the signs.
But the moment she whispered, “I believe you, Lily,” something inside the girl finally broke. She burst into tears, burying her face in her mother’s arms, shaking from years of unspoken terror.
And right outside the hospital doors, Daniel Whitmore was already in handcuffs—furious, screaming, demanding to see Lily—while officers forced him into the back of a squad car.
This time, he wouldn’t get anywhere near her.
The next few weeks were a whirlwind—medical appointments, interviews with investigators, court hearings, and countless hours of emotional support. Lily stayed in a protected shelter with her mother, away from anyone who might try to intimidate or influence the case.
Daniel Whitmore was formally charged with multiple felony counts, including child abuse, coercion, and statutory offenses. The evidence gathered at the hospital, combined with Lily’s statement and the timeline of events, was overwhelming. The prosecutor assured Catherine that Daniel would not be walking free anytime soon.
But legal justice was only one part of the journey. Lily’s emotional healing was something no court could accelerate.
She began trauma therapy with a counselor specializing in child abuse cases. At first, Lily barely spoke. She sat with her knees pulled up to her chest, her voice barely above a whisper, her eyes always scanning the room for danger.
But slowly—very slowly—she began to open up.
She started drawing again, something she used to love before fear took over her life. She played the piano in the shelter’s common room. She even laughed one afternoon when a therapy dog named Peanut climbed into her lap.
One day, during a follow-up appointment, Lily handed Dr. Hayes a small, folded note. Inside, written in shaky handwriting, were the words:
“Thank you for believing me.”
Dr. Hayes had to pause, breathe, and blink away tears.
Catherine, now separated from her husband and seeking full custody protections, attended every session with Lily. She faced her guilt head-on, focusing all her strength on rebuilding trust with her daughter. It wasn’t perfect, but it was real—and Lily could feel the difference.
Three months later, Daniel accepted a plea deal that ensured a long prison sentence. When the verdict was announced, Lily didn’t cheer. She didn’t smile. She simply squeezed her mother’s hand and whispered, “It’s over.”
But everyone who had helped her knew it wasn’t really over. Healing would take time—maybe years. But Lily was finally safe, finally heard, finally believed. And for the first time since she entered the emergency room, her future wasn’t defined by fear.
It was defined by hope.
If you were moved by Lily’s story, please leave a comment, share your thoughts, or tell me what kind of real-life stories you’d like to see next. Your engagement helps more people discover these powerful narratives.
My Foster Son Never Spoke a Single Word – Until the Judge Asked Him One Question

When Maren opened her home to a silent nine-year-old boy, she didn’t expect him to speak.
What she didn’t expect was how love could grow without words—through quiet routines, small mercies, and a presence that asked for nothing. Until the day, in a courtroom, he finally chose to be heard.
I didn’t say yes because I believed I could fix him.
I said yes because my house had been silent for too long, and I understood that kind of quiet. Mine came from loss. His came from something no one ever explained.

“He’s nine,” the caseworker told me, pausing deliberately. “He doesn’t speak, Maren. At all. Most families pass.”
“I’m not most families, Clara,” I said.
After three miscarriages and a marriage that ended with my husband admitting he couldn’t keep hoping, I had learned how to live with emptiness. He left with my expectations. My ability to love stayed.
It needed somewhere to go.
I didn’t wake up suddenly knowing I wanted to foster. It happened slowly—volunteering at the community center, helping at the food pantry. One afternoon, I found myself holding a child’s forgotten sweater, unable to put it down. That was when I knew.
When the paperwork arrived, thick and official, I pressed it to my chest. “You’ll come,” I told my reflection. “Whoever you are.”
So when they called about the boy no one wanted, I didn’t hesitate.
Evan arrived with one worn backpack and eyes that never stopped watching. He didn’t cry. He didn’t cling. He stood in the doorway like he was mapping exits.
“Hi,” I said softly. “I’m Maren.”
He walked past me and sat on the couch. I brought cocoa and cookies. He nodded once.
That was how we began.
I read aloud that night. He didn’t look at me, but he stayed. I didn’t push him to speak. I just lived beside him and left room for sound if it ever came.
I packed his lunches with notes. Some were silly. Some were gentle.
“I’m proud of you.”
“You’re doing great.”
“You’re the light I waited for.”
For weeks, they came back wrinkled or missing. One day, one was folded neatly on the counter, untouched. He’d kept it.
I cooked and talked while chopping vegetables, telling embarrassing stories. Sometimes his shoulders shook, like he was laughing quietly.
I pointed out birds on the porch, clouds shaped like ships, songs that reminded me of my mother. His silence didn’t feel empty. It felt careful. Like listening.
Over time, he sat closer. Waited by the door. Handed me my scarf if I forgot it. When I got sick one winter, I woke to water and a note beside the bed.
“For when you wake up.”
That was when I realized he watched over me, too.
Years passed. The house warmed. Evan hummed while doing chores. Once, when I sang terribly, he smiled. That smile told me everything.
People still asked.
“He still doesn’t talk?”
“Isn’t he too old?”
“Is something wrong with him?”
“He’ll speak when he’s ready,” I always said. “He just needs to stay.”
And he did.
When he was nearly fourteen, taller than me now, I filled out the adoption forms. I didn’t ask him outright.
“If you want this, just nod,” I said. “You don’t have to say anything.”
He nodded once.
The morning of the hearing, his hands wouldn’t stop folding the napkin.
“You’re not being sent back,” I told him. “Nothing about today changes us.”
The courtroom was bright and cold. Judge Calder sat at the bench, papers stacked high. Clara sat beside us.
“Evan,” the judge said gently, “you don’t have to speak. You can nod or shake your head. Do you understand?”
Evan nodded.
“Do you want Maren to adopt you? Do you want her to be your legal mother?”
He froze.
The silence stretched. My chest tightened.
Then Evan shifted. Cleared his throat.
“Before I answer… I want to say something.”
The room leaned in.
“When I was seven, my mom left me at a grocery store,” he said. “She said she’d come back. She didn’t.”
His voice shook, but he kept going.
“I moved around. People said I was strange. Too old. Not worth it.”
He looked at me.
“When Maren took me in, I thought she’d give me back too. But she stayed. She made cocoa. She read to me. She never forced me to talk.”
His hands twisted in his shirt.
“I stayed quiet because I was afraid if I said the wrong thing, I’d lose her.”
I was crying openly now.
“But I want her to adopt me,” he finished. “Because she’s already been my mom.”
The judge smiled softly. “I think that answers it.”
Outside, my hands shook as I reached for my car. Evan handed me a tissue.
“Thank you,” I whispered.
“You’re welcome, Mom,” he said.
That night, at bedtime, I reached for the old book.
“Can I read it tonight?” he asked.
I handed it over, my heart full.
May you like



I didn’t need him to say he loved me. I already knew. I had built a home someone chose to stay in.







